Rotation Recap: Cardiothoracic Surgery
This month I had the experience to work alongside a surgeon in his 70s who had been performing open heart surgery for over 40 years and his PA who had worked with him for 17 years. This month more than ever I understood the role of a surgical PA and the importance of being skilled as a first assist (and as a mind reader, since she was always 3 steps ahead). My preceptor in general surgery told me over and over again, a good assistant can make or break a surgery and cut the operative time by hours. This cardiothoracic dream team could complete a quadruple vessel CABG in 3 hours and I’m not exaggerating. Over the course of my rotation I had the opportunity to first assist in coronary artery bypass grafts, aortic valve replacements (both open and TAVR), countless carotid endarterectomies, abdominal aortic aneurysm repairs, pericardial windows, thoracotomies and VATS procedures, and learned the basics of endoscopic vein harvesting (a CRUCIAL skill for a PA with dreams of heart surgery!). I also rounded in the cardiac ICU and went to clinic once weekly for new patients and post-op appointments. The hours were intense and the work could be exhausting (one time we operated for over 10 hours only to have the patient ultimately be unable to come off of bypass), but I learned a lot and gained valuable technical skills, particularly with my suturing. It is absolutely incredible to saw open a chest and watch as the heart slowly stops beating as the bypass machine takes over. The lungs stop inflating and for one moment, everything is still. It’s even more incredible to take part in fixing a broken heart!
How To Prepare
Anticoagulation Nation – Take it all the way back to pharmacology (ugh) and review the different anticoagulation drugs. In particular, familiarize yourself with the mechanism of action, indications and contraindications, half lives, and availability of reversal agents. I have a handy chart that my inpatient medicine preceptor had me fill out and I’ve taken it to every rotation since. You can download that here. (It’s handwritten, just FYI.) Also brush up on measurements of anticoagulation (PT, PTT, & INR). These are important values to monitor in pre and post-op patients. Don’t forget that patients with mechanical valves require anticoagulation and regular INR checks for life!
Murmurs – Remember all those buzzwords that you learned in cardiac pathology? It can take a long time to be able to fully appreciate heart murmurs but it’s much easier if you’re able to recall where the murmur is best heard. For example, if your preceptor tells you that a patient has aortic stenosis, you will want to listen at the right sternal border, 2nd intercostal space. Ideally, you will also want to be able to tell if a murmur is systolic or diastolic. I won’t pretend like I ever heard the “click” of mitral valve prolapse or a “water hammer” murmur but I did at least learn when “that just don’t sound right!” This will serve you well in any role including primary care, emergency medicine, and pediatrics. You can always consult cardiology!
Coronary Angiography – One of my favorite things about heart surgery and the heart in general is that to see if something is wrong, all you have to do is look at it (either through CT angiogram or echocardiogram). I loved watching in real time as the blood flows (or doesn’t flow) and if the vessel is diseased enough, it’s clear where the lesion is. I used this powerpoint to brush up on the terminology and topography of cardiac angiography which is the most difficult part, in my opinion. It also teaches you how to interpret the report, which you should always check out in addition to your independent interpretation.

What To Expect
An Entourage – One thing I learned quickly about open heart surgery is that it takes A LOT of people to make it go smoothly. Once during a 2 vessel CABG/aortic valve replacement/MAZE procedure, the OR held an anesthesiologist, a CRNA, the surgeon, one PA first assisting at the chest, another PA harvesting the vein at the leg, myself, a scrub nurse, a circulating nurse, a perfusionist, a perfusionist student, two Edwards Lifesciences reps for the aortic valve, a rep for the MAZE equipment, and a patient care tech. Every single person is crucial (except us students) to making sure the procedure is successful. The rooms also become very crowded as the perfusion equipment is very large, there are tubes and lines EVERYWHERE, and other equipment like ultrasound machines are being rolled in and out. With this much going on, it’s critical to remember your OR etiquette and not contaminate ANYTHING! I cover that in more detail in my general surgery and plastic surgery recaps!
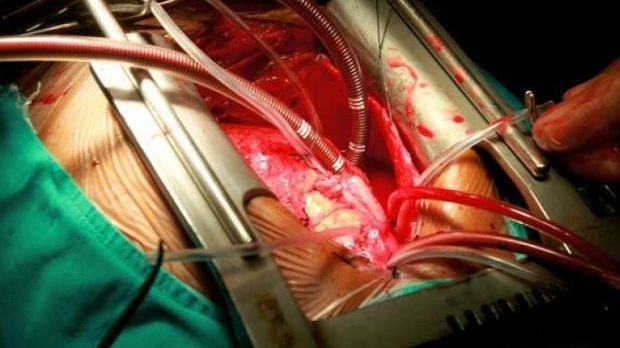
A Heartstopping Good Time – During the surgery, the patient will most likely be put on heart/lung bypass. The heart will be stopped and the lungs will not inflate for several hours. It felt like a true miracle watching all of this go down. Obviously, this is EXTREMELY intricate and detailed but I found it best to just keep in mind a basic understanding of what was happening at each step. One by one, the great vessels are cannulated and connected to the bypass tubes. The bypass machine oxygenates the blood, and returns it to the body (as the heart and lungs would). The heart is then stopped a potassium solution called “cardioplegia,” which is a solution of potassium. The heart is then cooled, decreasing the tissue’s need for oxygen. The perfusionist controls the bypass equipment, which controls the pressure, temperature, vessel of flow, direction of blood flow, and medications. Once the heart has completely arrested, it can be operated on. It’s CRAZY amazing, right!?
EVH – (Endoscopic Vein Harvesting) If you peruse PA job listings in cardiac surgery, most places want at least 1 year of EVH experience. (How one is supposed to get EVH experience as a new grad w/ no experience is baffling, but that’s for another day!) The main role of a PA in bypass surgery is to harvest the greater saphenous vein from the leg and prepare it to be anastomosed to the heart and aorta. It’s a delicate procedure requiring skill, concentration, and great tying skills! Practice tying down in tiny holes and practice pushing your knots down with your finger while avoiding tearing and pulling. If the graft leaks, it’s no good and it will probably be your fault! The photo below shows what you will be seeing on your screen as you harvest the vein with your endoscope.

As always, there is no way to be fully prepared for any rotation and the most important thing is to jump in with both feet and be willing to learn as you go. I always recap my rotations so if you’re heading into family medicine, emergency medicine, inpatient medicine, pediatrics, general surgery, OBGYN, psychiatry, or trauma/ICU, get the deets at these links! Feel free to leave your input in the comments and follow me on IG @coutureinclinic.